[JC Series] Critical Appraisal: MACMAN Trial - SHOWDOWN: Video vs Direct Laryngoscopy
MACMAN official citation:
Lascarrou JB, Boisrame-Helms J, Bailly A, Le Thuaut A, Kamel T, Mercier E, Ricard J, Lemiale V, Colin G, Mira JP, Meziani F, Messika J, Dequin PF, Boulain T, Azoulay E, Champigneulle B, Reignier J, for the Clinical Research in Intensive Care and Sepsis (CRICS) Group. Video Laryngoscopy vs Direct Laryngoscopy on Successful First-Pass Orotracheal Intubation Among ICU PatientsA Randomized Clinical Trial. JAMA.2017;317(5):483-493. doi:10.1001/jama.2016.20603

What was MACMAN's Clinical Question?
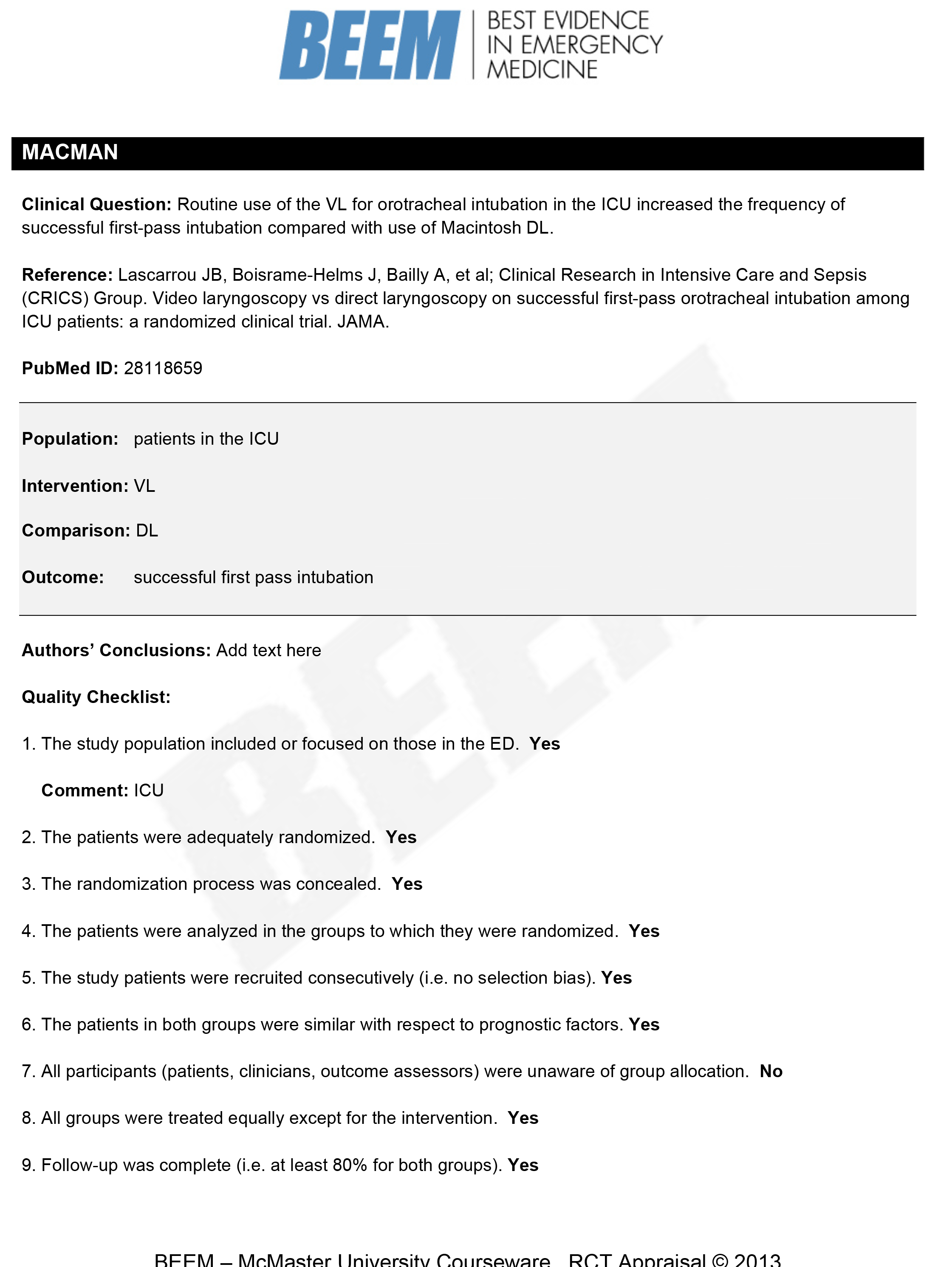
Does routine use of the VL for orotracheal intubation in the ICU increased the frequency of successful first-pass intubation compared with use of Macintosh DL
PICO Question
Population: patients in the ICU
- broad patient population
- examples of more narrow patient populations include: Severe ARDS or advanced stage COPD
Intervention: Video Laryngoscopy
Comparison: Direct Laryngoscopy
Outcome: successful first-pass intubation
- strong correlation between the frequency of complication such as hypoxemia, cardiac arrest, and death and the number of laryngoscopy attempts
- quantitative ETCo2/capnography to establish confirmation of successful attempt for objectivity
QUALITY CHECKLIST
1. The study population includes or focused on patients in the ICU? Yes
2. The patients were adequately randomized: Yes
- MACMAN randomized in blocks of 4
3. The randomization process was concealed: Yes
- software automatically allocated patients ensuring concealment.
4. The patients were analyzed in the groups to which they were randomized: Yes
- MACMAN did this well; they had one patient in the VL arm get DL
- Example: PROSEVA: Prone Positioning in Severe ARDS
- a few patients in the control were rescue proned.
- created a rescue prone positioning protocol
- included the rescue proned patient in the group they were randomized in
- Example: CESAR (ECMO in ARDS)
- patients in the ECMO arm did not always receive ECMO but were included in the ECMO group for analysis
5. The study patients were recruited consecutively (no selection bias): Yes
- patients were recruited from May to December 2015.
- Consider what was different about ICU care during that period of time.
- For example CESAR enrolled patients from 2001 to 2006.
- ARDSnet was published in 2000 (ARMA trial)
- For example CESAR enrolled patients from 2001 to 2006.
- Determine if the care you think those patients received during that time matches your current practice
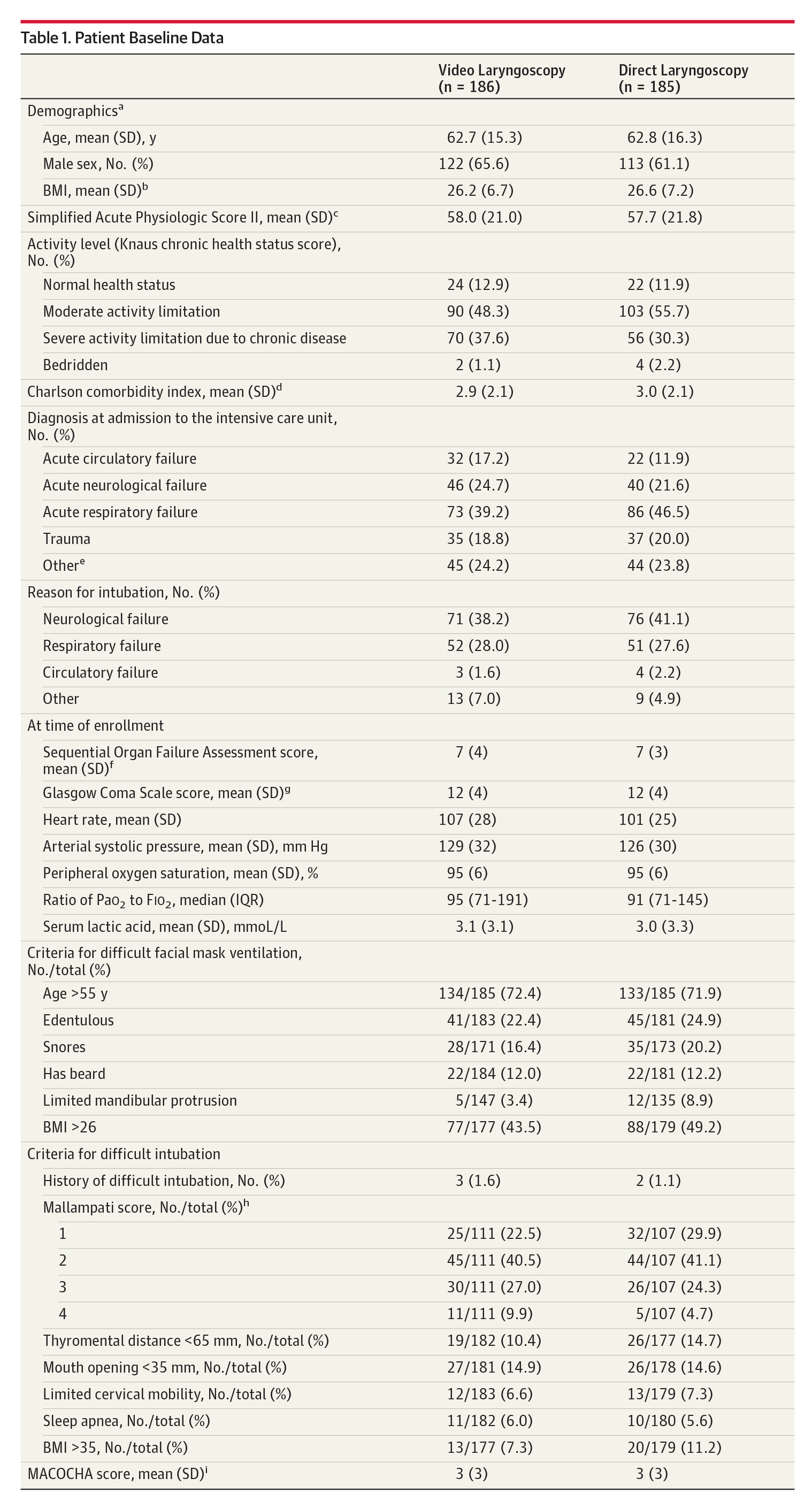
6. The patients in both groups were similar with respect to prognostic factors: Yes
- Ask yourself does the patients demographics match my patient population? Age? sex? weight? and severity of illness?
- Most studies use SOFA or APACHE II
- MACMAN used SOFA (Sequential Organ Failure Assessment Score)
- MACMAN Table 1
- Age mean 62; mean BMI 26
- SOFA 7
7. All participants (patients, clinicians, outcomes assessors) were unaware of group allocation: NO
- The clinician intubating the patient knew if they using a DL or VL and can't be blinded.
- Example of classic double blinded study
- SPLIT trial comparing Plasmalyte to Normal Saline
- plain labeled 1L bags of fluid either labeled "Fluid A or Fluid B" and the fluids were "macroscopically indistinguishable"
- SPLIT trial comparing Plasmalyte to Normal Saline
8. All groups were treated equally except for intervention: Yes
- RCT's try to focus on one intervention or therapy and keep everything else the same
- retrospective and observational studies cannot control variables as well
- Example: Noninvasive Ventilation to prevent reintubation
- "Prospective before-after study"
- The control group was enrolled from 2005-2006
- the NIV cohort was enrolled from 2010-2012
- Example: Noninvasive Ventilation to prevent reintubation
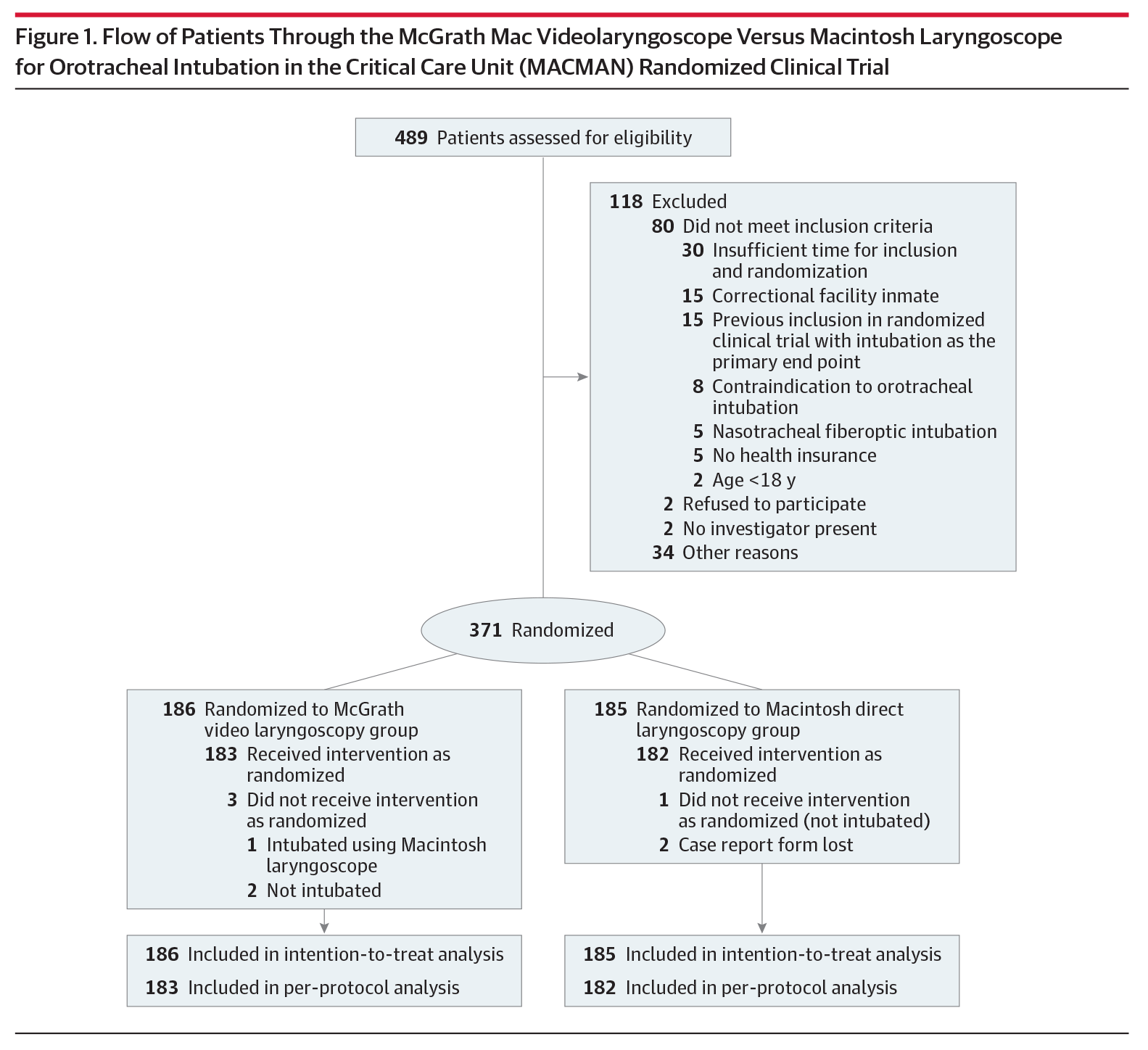
9. Follow-up was complete (at least 80% for both groups): Yes
- MACMAN: Figure 1
10. All patient important outcomes were considered: Yes
- what outcomes do I care about for my patients when considering adopting this therapy?
- Is this the right primary outcome measure?
- Mortality is common
- Objective data points such as FEV1 in pulmonary
- Subjective data points such as 6-minute walk tests in pulmonary
- Secondary outcomes for MACMAN
- Cormack Lehane view
- bougie use
- complications including mild to mod and severe
- difficult intubations
- reason for intubation failure
- airway manuvers used such as Selick manuver
11. The treatment effect was large enough and precise enough to be clinically significant: Yes
- Determine expected outcomes for intervention and comparison groups
- Power: Calculate how many patients they need to see the change in outcome in the intervention group taking into account Type 1 and Type 2 error (future podcast!)
- MACMAN calculated they needed at least 370 patients to be adequately powered
- After exclusion they had 371 patients
KEY RESULTS:
- primary outcome:
- VL 67.7%
- DL 70.3%
- no significant difference (p = 0.60)
- no difference after adjusting to operator expertise

- Grade 1 or 2 Cormack Lehane more common in VL group
- bougie used more often during first pass in VL
- most first attempts done by nonexpert intubators
- first attempts more successful in both groups if expert intubating
- no time difference in successful intubations (2 min to 2.5 min)
- higher percentage of severe complications in VL group (9.5 vs 2.8%)
- no sig difference in mild to mod comps
- other important typical secondary outcome measures in the ICU were looked at and did not differ:
- ICU LOS
- duration of vent
- SOFA scores on different days of ICU stay
- ICU mortality
- 28 day mortality
Author's Conclusions:
VL compared to DL did not improve intubation rates and was actually associated with higher rates of severe life threatening complications
Our conclusions
- VL vs DL debate rages
- Quality large multicenter RCT published in high impact Journal
- well powered to prove primary outcome
- well designed trial
- Be cognizant of your biases when reviewing papers
- Used McGrath only which is a handheld VL with smaller screen
- not neccesarily applicable to other VL's
- Used McGrath "indirect" 3 or 4 blade
- did not use hyperangulated blade
- VL able to get better views but not better success
- it's possible to get views that are too good: Kovac's Sign

- Higher severe hypoxemia in VL group
- good view makes you falsely comfortable
- intubators will attempt multiple times
- vulnerable to keep trying same plan over and over
- Elaine Bromiley Case : LITFL Lessons from Elaine Bromiley Case
- good view makes you falsely comfortable
- Ardent VL or DL supporters: debate frequently breaks out on twitter.
The Bottom Line
- Use what you are best at: DL or VL
- Practice getting good at both
- No evidence to support VL over DL based on this trial
- higher rates of severe complications with VL warrants more study
Clinical Application
- Utilizing VL more than DL in training
- do we back away from teaching VL first?
- Is VL better for teaching?
- If using VL: recognize its limitations
- will get great look; may not always be able to pass the tube
- know when to move on the plan B, C, or D
Supplemental Material mentioned in the Episode