

infectious disease
Sepsis
Sepsis is A life threatening condition that arises when the bodys REPSONSE to infection causes injury to its own organs. The bodys response varies per person and is not necessarily correlated with the amount of insult someone undergoes. It is something we seeing in virtually all ICU patients; it is truly a core topic that you MUST have a in-depth understanding of. Inappropriately treating a septic patient early on can kill someone. As a trainee, you will go over the early definitions of sepsis and how to treat it; once you have a solid understanding of these, you can go over the newer definitions.
History
The word "sepsis" is derived from the Greek word that means "rot". In around 400 B.C., Hippocrates first described sepsis as "the decay of biologic materials in the colon leading to dysregulated body humors". Later, in 200 A.D. Galen - a physician who specialized in draining abscesses - described the "formation of pus" absolutely necessary for wound healing. It was a phenomenon that both the Romans and Greeks recognized - specifically, the Romans believed that invisible creatures within swamps released putrid fumes called "miasma" that caused infection. While they recognized the idea behind sepsis they incorrectly dealt with it by removing as many swamps as possible instead of stopping the spread of infection with handwashing/sterile technique.
Later, once germ theory was discovered (e.g. time of Pasteur), the idea of bacteria causing infection became more widespread and sepsis was known as systemic infections caused by an overwhelming amount of a pathogen ("blood poisoning").
Even later, as antibiotics made their way into the world people started realizing that even though we were removing the pathogen, people were still dying. Ultimately this started the idea that in sepsis the host is killing the host, not the pathogen.
Modern Day
The first general definition of sepsis was created in 1992 by SCCM/Chest. It was formed by an international consensus panel due to the high morbidly and mortality that sepsis held. They defined SIRS (systemic inflammatory response syndrome); severe sepsis (SIRS complicated by acute organ dysfunction) and septic shock (SIRS complicated by hypotension, hyperlactemia).
In 2001 Emmanuel Rivers came up with Early Goal Directed Therapy. This was the first standardized "guideline" on how to treat SIRS, severe sepsis and septic shock. It was derived from cardiac surgery "goal directed therapy" which had proven to decreased morbidity and mortality in post-surgical patients. This includes the three hour and six hour bundle.
In 2003, a 2nd consensus was held to look at the guidelines, specifically after they noticed SIRS had a low specificity for infected patients. In this definition they essentially agreed with the 1992 definition but removed sepsis; kept severe sepsis/septic shock.
The most recent guidelines, SEPSIS-3, was defined in February of 2016. These included newer information with the 1992 guidelines be much more outdated. SEPSIS-3 scraps the old definition and instead defines sepsis as "organ dysfunction secondary to a dysregulated host response to infection". It defines sepsis as a SOFA, or sequential organ failure assessment, score of 2 or more (or a qSOFA of >2/3), with the SOFA score being much more specific for infection than SIRS. It removes the idea of severe sepsis and defines septic shock as a LA>2 or MAP<65 after adequate fluid resuscitation.
Resources to complete:
KNOW Sepsis Pulmcast Resource Page
Marino 3rd ed: Ch. 40-44; 4th ed: 39-41
Rivers Early Goal Directed Therapy article [NEJM 2001]
PROCESS/PROMISE/ARISE [NEJM 2014] - no benefit of EGDT compared to usual care
PROCESS (USA) - Summary / PDF of Article
PROMISE (England) - Summary / PDF of Article
ARISE (Aus/NZ) - Summary / PDF of Article
TRISS - Summary / PDF of Article
Surviving Sepsis Guidelines 2021
Pulmcast Sepsis Multicast Episode 1
Pulmcast Sepsis Multicast Episode 2
Pulmcast Sepsis Multicast Episode 3
Pulmcast Sepsis Multicast Episode 4
Pulmcast Sepsis Multicast Episode 5
Pulmcast Sepsis Multicast Episode 6: Chad Case Sepsis SMACKDOWN
Emcrit Practical Evidence Podcast 015: Surviving Sepsis Guidelines 2016
Lactate Clearance vs Central Venous Oxygen Saturaiton as Goals of Early Sepsis Therapy - a RCT
Bacteria and Antibiotics
In the ICU, infections are quite common, and when they become severe, they often lead to something we all fear - sepsis. Sepsis is a severe bodily response to infection, and it's a major concern in hospitals because it can be life-threatening. Treating sepsis involves controlling the source of the infection, and one crucial step is getting patients on the right antibiotics. But which antibiotics should we use? Let's break it down for someone who isn't familiar with antibiotics and bacteria.
In the ICU, we're concerned about a few different types of bacteria. We group them into categories:
Gram Positive: These are bacteria like staph infections.
Anaerobes: These are bacteria that don't need oxygen to thrive.
Gram Negative: These are bacteria like E. Coli.
We also consider where the infection is in the body:
Gram Negative Pathogens Above the Diaphragm: This includes infections like pneumonia (pneumococcus, H, influenza, pseudomonas, staph aureus).
Gram Negative Pathogens Below the Diaphragm: Think about infections in the abdomen; there are a lot of different bacteria to worry about here. This includes bacilli normal to the bowel; belong to the family Enterobacteriacae (“Enteric organisms”), gram negative rods. Generally, it’s a lot of anaerobic bacteria.
Urinary Tract Infections (UTI): Common culprits here are E. Coli, proteus mirabilis, Klebsiella pneumonia.
Intra-abdominal Pathogens: These are the bacteria that can cause trouble in your gut. Think urinary tract bacteria, plus interstitial anaerobes with includes Bacteroides fragilis, Clostridium Tetani, Clostridium difficile, bacteroides disastonis, bacteroides ovatus, bacteroides thetaiotamicron, fusobacterium
Pelvic Infections: Think about sexually transmitted infections like chlamydia trachomatis, gardnerella.
We also need to be aware of drug-resistant organisms - MRSA (methicillin resistant staph auerus), MSSA (methicillin sensitive staph auerus), CRO (carbapenem resistant organisms). With these bacteria in particular you need to be judicious about using antibiotics that appropriately treat them.
When it comes to treating infections in the ICU, two antibiotics you'll often hear about are Vancomycin and Zosyn (piperacillin/tazobactam). Vancomycin is effective against many Gram-positive bacteria, including those resistant to antibiotics (like MRSA). Zosyn, on the other hand, covers a broad range of Gram-negative bacteria and even some pesky pseudomonal infections.
Vancomycin covers: MRSA, some staph infections, and certain enterococcus bacteria.
Zosyn covers: MSSA, some enterococcus bacteria, streptococcus, anaerobes, Gram-negative cocci, E. Coli, Klebsiella, Proteus Mirabilis, and some pseudomonal infections.
The good thing is that Vancomycin and Zosyn cover most of the common bacteria we encounter in the ICU (at least for now). See the table below.
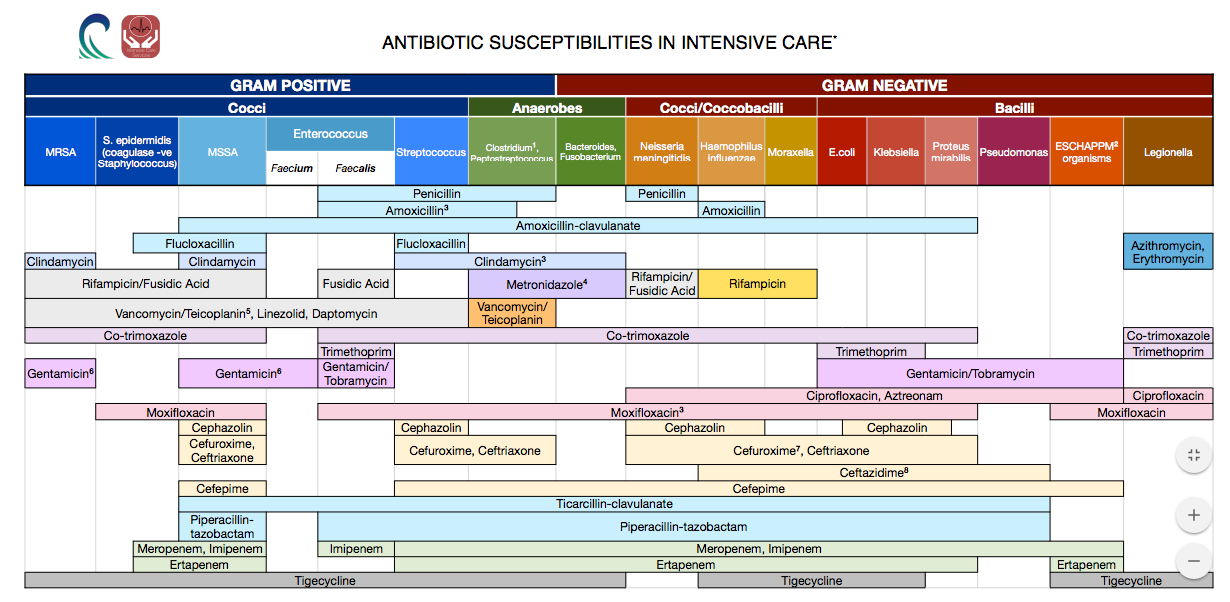
More detailed chart; some of these medications are ID only and not normally used by non-infectious disease providers.

Better chart for non-ID providers (the ICU).
Some specific trends you will see:
You will sometimes see patients be on Ancef (Cefazolin) for staph coverage peri-operatively
You will often see transplant patients on Bactrim for PCP coverage
Certain medications can only be ordered if ID is consulted
And some common medications and their effects:
Vancomycin can precipitate/worsen renal failure
Zosyn can cause thrombocytopenia
All About Cultures
In the ICU, the ability to accurately diagnose and treat infections is crucial for patient care and outcomes. Culturing biological samples is a fundamental tool in the diagnostic process, providing valuable information about the presence of pathogens and their susceptibility to antimicrobial agents. When it comes to getting cultures in our ICU, here are the most common you will see:
Blood cultures (usually as part of sepsis bundle)
Urine cultures (a UTI can only be diagnosed with culture; not with a urinalysis, although a UA could lead you to suspect)
Respiratory cultures - sputum expectorated (patient expectorates/spits manually) or BAL (bronchioaleveolar lavage during bronchoscopy)
Wound cultures
Stool Cultures
Blood Cultures
Blood cultures involve the collection and incubation of a patient's blood sample to detect the presence of microorganisms, such as bacteria or fungi, in the bloodstream. The primary goal of blood cultures is to identify the causative agent responsible for the infection, which helps guide appropriate antibiotic therapy.
A positive blood culture result indicates the presence of microorganisms in the bloodstream. It is crucial to differentiate between true bloodstream infections and contamination during sample collection or processing. The interpretation of positive blood culture results involves considering several factors:
Identification of Pathogens - The first step in interpreting a positive blood culture is identifying the microorganism responsible for the infection. This is typically done through laboratory techniques such as Gram staining, subculturing, and biochemical tests. Identifying the pathogen helps guide appropriate antimicrobial therapy and infection control measures.
Quantification of Growth - The quantification of microbial growth in blood cultures is essential for determining the clinical significance of the infection. The number of colony-forming units (CFUs) per milliliter of blood can provide insights into the severity of the infection. Higher CFU counts often indicate a more significant infection, while lower counts may suggest contamination or a less severe infection.
Time to Positivity - The time taken for a blood culture to become positive can provide valuable information about the type of microorganism causing the infection. Some pathogens, such as Staphylococcus aureus, grow rapidly and can cause a positive blood culture within a few hours. Other organisms, like slow-growing fungi, may take several days to show growth. Time to positivity can help guide empirical antibiotic therapy and narrow down the potential pathogens.
Polymicrobial Infections: In some cases, blood cultures may yield multiple different microorganisms, indicating a polymicrobial infection. Interpreting polymicrobial infections can be challenging, as it requires identifying the significance of each organism and determining their individual roles in the infection. Polymicrobial infections are often associated with more severe clinical outcomes and may require a tailored treatment approach.
A negative blood culture result suggests the absence of microorganisms in the bloodstream at the time of sample collection. However, it is important to note that a negative result does not completely rule out the presence of an infection. Several factors can contribute to false-negative blood culture results:
Timing of Blood Culture Collection - The timing of blood culture collection is crucial for maximizing the chances of detecting a bloodstream infection. In some cases, the pathogen may have already been cleared from the bloodstream by the time the blood culture is obtained. Repeat blood cultures may be necessary if clinical suspicion of infection remains high despite an initial negative result.
Prior Antibiotic Therapy - The administration of antibiotics before blood culture collection can significantly impact the sensitivity of the test. Antibiotics can suppress the growth of microorganisms in the bloodstream, leading to false-negative results. It is important to consider the timing and duration of antibiotic therapy when interpreting blood culture results.
Fastidious Organisms - Some microorganisms have specific growth requirements and may not be detected by standard blood culture techniques. Fastidious organisms, such as certain types of bacteria or fungi, may require specialized culture media or longer incubation periods to grow. If there is a strong clinical suspicion of infection with a fastidious organism, additional diagnostic tests may be necessary.
Low Inoculum Infections - Infections with a low inoculum, where the number of microorganisms in the bloodstream is very low, can result in false-negative blood culture results. Low inoculum infections are more common in certain types of infections, such as endocarditis or infections caused by slow-growing organisms. Clinical correlation and consideration of other diagnostic tests may be necessary in such cases.
Contamination of blood cultures can occur during sample collection, processing, or transportation, leading to false-positive results.
Skin Flora Contamination - Contamination with skin flora, such as coagulase-negative staphylococci or diphtheroids, is a common cause of false-positive blood cultures. These organisms are part of the normal skin microbiota and can contaminate blood cultures during sample collection. Clinical correlation, repeat blood cultures, and consideration of other diagnostic tests can help differentiate between contamination and true infection.
Laboratory Artifacts - Laboratory artifacts, such as improper handling or processing of blood cultures, can lead to false-positive results. Contamination can occur due to inadequate disinfection of culture bottles or improper aseptic techniques during subculturing. Quality control measures and adherence to standardized protocols are essential to minimize the risk of laboratory-related contamination.
Consistency with Clinical Presentation - Evaluating the consistency of blood culture results with the patient's clinical presentation is crucial in differentiating contamination from true infection. If the patient does not exhibit signs and symptoms consistent with an infection, and other diagnostic tests are negative, the possibility of contamination should be considered.
Interpretation of Blood Cultures
GRAM POSITIVE PATHOGENS
Enterococcus faecalis
Often a GI pathogen
If it is found in urinary culture, often associated with nosocomial and/or obstruction, urinary catheterization, or instrumentation
Also can be meningitis, wound infections, endocarditis
Associated with endocarditis if found in the blood (e.g. Enterococcus faecalis bacteremia)
Usually susceptible to Penicillin; also covered by Vancomycin
Enterococcus faecium
Associated with endocarditis if found in the blood (e.g. Enterococcus faecium bacteremia)
The most important distinguishing feature between faecalis and faceium:
Faceium is often resistant to Penicillin and can be resistant to Vancomycin: so you need ID consult for Dapto/Linezolid
Listeria monocytogenes
Gram positive rod in chains
Associated with meningitis, immunosuppressed older adults and pregnant women
Treat with Ampicllin/Penicillin combined with Gentamicin
Should consult ID if you find this
Staphylococcus spp
Stands for “Staphylococcus Species” - just tells you its Staph, doesn’t mean theres two things, its just confirming Staph
Staphylococcus aureus
In general, Staph aureus in the blood is a big deal
Staphylococcus epidermidis
It is often contamination in blood cultures but can also be legit, found on the skin
Staphylococcus lugdunensis
Can be on the skin but associated with prosthetic joint or prosthetic valve infections so don’t overlook it/call it a contaminant until you are sure
Streptococcus spp
Stands for “Streptococcus Species” - just tells you its Strep, doesn’t mean theres two things, its just confirming Strep
Streps are truly complicated - the families can be complex.
Streptococcus pneumoniae
In our practice often associated with community acquired pneumonia. Bad cases can cause meningitis
Beta hemolytic streps:
Streptococcus agalactiae
Group B strep; not commonly seen in ICU, big deal in pregnant women, but can cause soft tissue infections and UTIs
Streptococcus pyogenes
Group A hemolytic strep, important for ICU because it can cause toxic shock syndrome/necrotizing fasciitis
GRAM NEGATIVE PATHOGENS
Acinetobacter calcoaceticus-baumannii complex
Gram negative: hospital. Commonly seen in VAPs, hospitalized patients; high levels of resistance. Consider ID consult
Bacteroides fragilis
Anaerobic gram negative found in intestinal flora- look for a bowel perf!
Haemophilus influenzae
In our practice often associated with community acquired pneumonia. Bad cases can cause meningitis
Neisseria meningitidis
Patient with splenectomy are a high risk for meningitis due to this
Pseudomonas aeruginosa
Common hospital/nursing home acquired pathogen and a common cause of VAP. Quickly develops resistance to antibiotics.
Stenotrophomonas maltophilia
Almost always associated with VAP
Enterobacteriaceae: If this is positive, it just means it’s in the gram negative category (see below)
This is a family of gram negative bugs; they can be in the urinary tract, GI tract, and occasionally respiratory system. A lot of these are common and you’ll see in many different types of patients.
Enterobacter cloacae complex
Escherichia coli
Klebsiella aerogenes
Klebsiella oxytoca
Klebsiella pneumoniae group
Proteus spp
Salmonella spp - associated with GI illness
Serratia marcescens - think about line infections in paticular on top of typical gram negative sites
FUNGAL PATHOGENS - if these are in the blood, consult infectious disease. This is bad.
Candida albicans
Candida auris
Candida glabrata
Candida krusei
Candida parapsilosis
Candida tropicalis
Cryptococcus neoformans/gattii - very very bad, worry about patient being severely immunocompromised (e.g. AIDS)
Resistance Genes:
CTX-M: Extended-spectrum beta-lactamases, or enzymes that confer resistance to most beta-lactam antibiotic (ESBL)
KPC: Carbapenemase resistant (CRO)
mec A/C: methicillin resistant, could be MRSA or MRSE
NDM: Carbapenemase resistant (CRO)
vanc A/B: VRE
IMP: Carbapenemase resistant (CRO)
mcr-1
mecA/C and MREJ: MRSA
OXA-48-like: Carbapenemase resistant (CRO)
VIM: Carbapenemase resistant (CRO)
Urine Cultures
When a urine sample is sent to the laboratory for culture, it undergoes a series of tests to identify and quantify any microorganisms present. The laboratory report typically includes several key components that aid in interpreting the results:
Culture Growth: The report will indicate whether there is growth of microorganisms in the urine sample. If no growth is observed, it suggests that the sample is sterile and free from significant bacterial or fungal pathogens. However, it is important to note that the absence of growth does not rule out the possibility of a UTI, especially in cases where the patient has been recently treated with antibiotics.
Colony Count: If there is growth in the urine culture, the report will provide the colony count, which represents the number of microorganisms present in the sample. Colony counts are usually reported as colony-forming units per milliliter (CFU/mL). Higher colony counts generally indicate a higher likelihood of infection, although the specific threshold for diagnosing a UTI may vary depending on the patient's clinical presentation and risk factors.
Identification of Pathogens: The laboratory will identify the specific microorganisms present in the urine culture. This information is crucial in determining the causative agent of the infection and guiding appropriate antibiotic therapy. Common pathogens associated with UTIs include Escherichia coli, Klebsiella pneumoniae, Proteus mirabilis, and Enterococcus faecalis.
Antimicrobial Susceptibility Testing: The report may also include information on the susceptibility of the identified pathogens to various antibiotics. This helps guide the selection of appropriate antimicrobial therapy, taking into account the local resistance patterns and the patient's individual factors such as allergies and previous antibiotic exposure.
Interpreting urine culture results requires a comprehensive understanding of the patient's clinical presentation, risk factors, and the specific characteristics of the microorganisms identified. Here are some key considerations when interpreting urine culture results:
Symptoms and Clinical Presentation: The presence of significant bacteriuria (bacteria in the urine) alone does not necessarily indicate a UTI. It is essential to correlate the culture results with the patient's symptoms such as dysuria (painful urination), frequency, urgency, and suprapubic pain. The presence of symptoms along with positive culture results supports the diagnosis of a UTI.
Colony Count: The colony count is an important factor in determining the significance of the bacterial growth. In general, colony counts of ≥10^5 CFU/mL in midstream clean-catch urine samples from symptomatic patients are considered indicative of a UTI. However, lower colony counts (e.g., ≥10^3 CFU/mL) may be significant in certain patient populations, such as those with indwelling urinary catheters or immunocompromised individuals.
Pathogen Identification: The specific microorganism identified in the urine culture helps guide targeted antibiotic therapy. Different pathogens have varying levels of virulence and antimicrobial resistance patterns. For example, Escherichia coli is the most common cause of community-acquired UTIs and is typically susceptible to first-line antibiotics such as trimethoprim-sulfamethoxazole and fluoroquinolones. On the other hand, Enterococcus faecalis is often associated with healthcare-associated UTIs and may exhibit resistance to multiple antibiotics.
Antimicrobial Susceptibility: The antimicrobial susceptibility testing results provide valuable information on the effectiveness of various antibiotics against the identified pathogens. It is important to select antibiotics to which the pathogen is susceptible to ensure optimal treatment outcomes. However, it is crucial to consider local resistance patterns and individual patient factors when making antibiotic choices.
Positive urine culture results, along with compatible clinical symptoms, support the initiation of antibiotic therapy. The choice of antibiotics should be guided by the identified pathogen and its antimicrobial susceptibility profile. Empirical therapy may be initiated initially, followed by adjustment based on the culture results and susceptibility testing.
Urine samples can easily become contaminated during collection, leading to false-positive results. Proper collection techniques and adherence to sterile procedures are essential to minimize the risk of contamination.
Respiratory Cultures
It is important to note that this section is referring to BACTERIAL respiratory cultures. You will see another test in our ICU, called a “Respiratory Panel”, which tests for viral pathogens. A respiratory panel is obtained with a nasal swab. Commonly, patients awaiting the results of a respiratory panel will be under enhanced modified precautions (contact, droplet).
In the context of bacterial respiratory cultures, the obtained results can typically be categorized as either quantitative or qualitative.
Quantitative results are expressed in terms of colony forming units per milliliter (cfu/mL) or cubic centimeter (cfu/cc), such as "10,000 cfu/cc of E. Coli." When assessing a bronchoalveolar lavage (BAL) sample, if the bacterial count exceeds 10^3 (greater than 1,000), it is likely to be considered positive. Similarly, a mini-BAL sample is considered positive if the bacterial count is at least 10^4 (greater than 10,000), while a sputum sample is indicative of positivity if the bacterial count reaches at least 10^5 (greater than 100,000). However, it is crucial to exercise clinical judgment and correlate these findings with other clinical data, such as procalcitonin levels, signs and symptoms, sputum production, and additional relevant information.
Qualitative results describe the growth of bacteria in a more descriptive manner, such as "moderate growth of E. Coli." In most cases, medical practitioners opt for treatment regardless of the bacterial count because the presence of a significant quantity of bacteria in the lungs is abnormal and necessitates intervention.
In the interpretation of these cultures, the hospital's laboratory often labels the findings as "normal respiratory flora" when they detect the presence of typical, non-pathogenic bacteria. This distinction highlights the importance of clinical context when evaluating respiratory culture results to ensure appropriate treatment decisions are made.
Stopping Antibiotics
Determining when to stop antibiotics is a complex decision that healthcare professionals in the ICU must carefully consider. Antibiotics are a vital tool in treating infections, but their prolonged use can lead to antibiotic resistance and other complications. In the ICU, the decision to discontinue antibiotics is guided by various factors, including clinical improvement, resolution of infection-related symptoms, laboratory markers such as white blood cell counts and inflammatory markers, and, importantly, the results of microbiological cultures. Once it is evident that the infection has been adequately treated, continuing antibiotics may do more harm than good. ICU teams are trained to strike a delicate balance, ensuring that antibiotics are appropriately continued for active infections while avoiding unnecessary antibiotic exposure, ultimately contributing to more effective and responsible antibiotic stewardship in critical care.
Resources to complete:
CLABSI/CAUTI
HCAP/HAP/VAP/Severe CAP
FCCS Ch. 11
Marino 3rd ed: Ch. 41; 4th ed: Ch 29
Medcram: Ventilator Associated Pneumonia (VAP)
Antibiotics
Antimicrobials: What, What, and for How Long
Antimicrobial Therapeutics in Critical Care
Pulmcast: Deep Dive Procalcitonin
Choosing and Deescalating Antibiotics (Youtube Video)
30 Minute Review On Choice of Antibiotics for Sick Patients (Youtube video)
Guidance for managing patients with allergies to beta lactam antibiotics other than penicillin