
nursing pearls for the new APP
For those fresh out of school entering the hospital environment, navigating the basics of inpatient medicine can be a bit of a challenge. The terminology used and the equipment in the room can seem foreign at first. While we typically aren't the primary individuals handling pumps, IVs, and the like, it's important to familiarize ourselves with these elements so we can communicate effectively with our colleagues and understand any obstacles in patient care.
Mediation Formulations
Medications often come IV push (IVP), continuous or piggybacked.
Piggyback Medications: A piggyback serves as a secondary line that temporarily interrupts your primary line to administer another medication automatically. For instance, if you have keppra on piggyback, it will run for 15 minutes on its own, and then the primary IV fluids will resume automatically. The purpose is to conserve channels (which can be in short supply) and overall be less bothersome, freeing up an IV site. You don't need to manually turn it off when it's done, and it won't beep at the patient.
Continuous Infusions: This involves a single primary line.
IVP (IV Push): You administer the medication in a single push, usually followed by a flush to clear the line tubing.
IV Compatibility
Nurses typically determine this by referencing a resource like lexi-comp. Not all medications can be mixed together. For example, amiodarone must run on its own and be filtered, while vasopressors can be administered together in the same line. Insulin must also be administered separately.
Compatible medications are connected at a "y-site." However, you must be cautious with the y-sites themselves, which are located sequentially down the IV tubing from closest to the patient to farthest from the pump. If you have vasopressors and fluids going simultaneously, it can push the vasopressor into the patient if you're not careful about the location of the y-site.
IV pumps

At Piedmont, we use Alaris pumps. The main part of the pump you interact with is called the brain, and the channels are where the IV lines run; they're programmed for the drugs running through them. There are two programming modes: critical care and acute care. On the floor, pumps are programmed for acute care, limiting the medications that can be administered.
You cannot have more than four channels on one brain; it doesn’t matter what side they are on.
Keep an eye out for error alerts:
Air in line: there is a bubble potentially in the actual channel itself, this will stop medication from being delivered.
Tubing can be dry, bubble can be somewhere; champagne bubbles are okay but not big bubbles. To get it out the nurses will thump it/tap it with their fingers/thumb.
Occluded line: often with AC IVs when a patient bends their arm or the tubing gets pinched in side rails.
Infusion complete: the volume set in the channel has been delivered; indicates that the pre-set volume has been delivered; make sure this isn't your vasopressor, and if it is, notify your nurse.

An open channel where you place the IV tubing

The brain will list what medications are running and what their dosages are (what they’re running at)

Example of a “Y-site” (where two medications join) - this is propofol and fentnyl

Multiple “Y-Sites” with the one on the right closer to the patient and the one on the left farther away (and unused)

The clamp - somewhat of a moot point if there is a channel above it, but if a bolus is running this helps dictate the flow. Move it down to clamp it (slower flow) and move it up to open it up (faster flow)
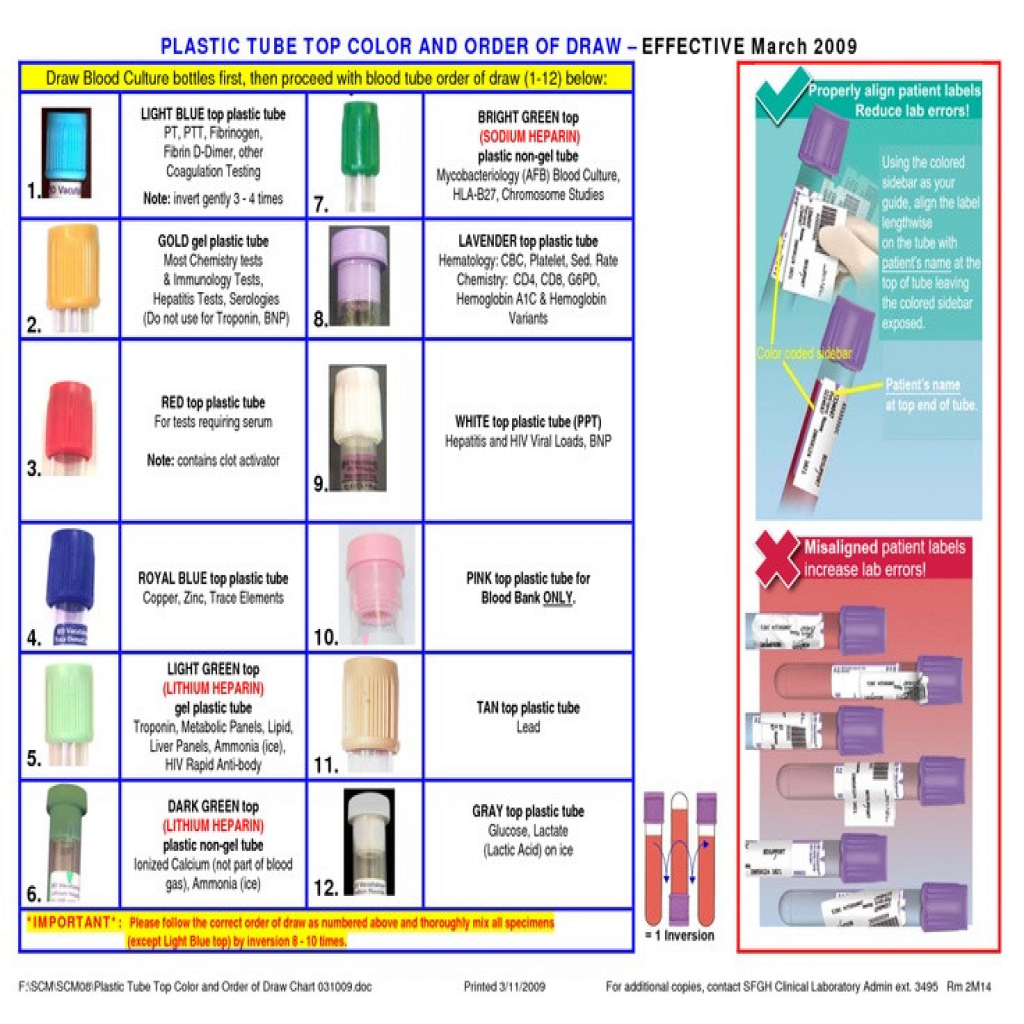
Lab Draws
When you draw blood for a lab there are many different color tube tops available. Each color references a different “mixer” inside of it that enables it to be processed correctly. Often, the specific tube that is needed is referred to by the color top it is. For example, if someone called out “I need a pistachio”, it means you need a light green topped tube, not the nut you eat.
Some labs require special handling. Lactic acid and ammonia must be drawn and immediately placed on ice. Ionized calcium tubes are dark green, unlike most other chemistry levels, which use pistachio-colored tubes.
When a lab is ordered, a label is generated and attached to the tubing, specifying the type of test, tube color, and any special instructions. If you forget to order a lab, you can sometimes "add it on" to the blood already sent down, but this is limited to labs in the same tube color. EPIC will usually tell you if add-on is available.

Yankauer
random Nursing Terms
INT = autoclaves = “intermittent”, basically just means non-used IV
Trialysis = central line (three ports)
Straight cath = intermittent emptying of the bladder
Nurse draw = nurses able to draw labs instead of lab tech
Dinomap = portable vital sign monitor w/automatic blood pressure, often blue in color
“Pressure bag” - they actually put a thing around the medication/fluid that places pressure on it and causes it to go in very fast; must request this, if you don’t have one can squeeze with hands
OGT = oral gastric tube, placed in mouth usually on vented patients
NGT = nasogastric tube; placed in nose, larger, you can suction
DHT = dobhoff tube, essentially a smaller OGT/NGT; super tiny and can only do feeds in it, cannot suction
TPN/PPN = forms of nutrition; one is peripheral (PPN) one is central (TPN), gives nutrition and electrolytes, nursing/dietary/pharmacy collaborates. Can increase risk of bacteremia
Rectal tube = tube that goes off anus to collect feces. Do not use on GIB, abdominal infections, anyone at high risk of perf/bleeding
Purewick = for women; catches the pee and sucks it up, sits between the legs. Looks like a huge tampon
Condom cath = non-invasive condom that drains pee from the male; attached to a foley bag/tubing
IPCs (intermittent pneumatic compression) = leg squeezers, prevent clots
Dial-flow: special tubing often in the ED where you can control continuous flow so you don’t need a brain/channel to use it; but if you bend arm/etc it does not alarm because there’s no computer to alarm
Admixture: you can add two things in the same bag, usually mixed by pharmacy
Yankauer = apparatus that attaches to suction tubing and is your handle
Curos caps = cap that has alcohol embedded into it and sits on the line while not being used; keep the y-sites clean so you don’t have to scrub it every time, must place a new one every time
Pigtail = squishy rubber band thing you pull to flush anything your transducing (think a-lines)
Claves = attaches to attachments on line, blood/meds can’t come out but you can push meds in
Other Pearls
Places for IVs - anywhere you can get them; but wrist/forearm preferred, AC can be annoying for patient
Blood cultures can’t be drawn from IVs/CVLs -must be stick
Switching from regular to quad strength vasopressors or switching from regular IV to central line IV - must change IV tubing!
Some oral medications can be crushed down OGT/NGT once patient is intubated. You cannot crush extended-release medications, as it makes the pharmacokinetics completely unpredictable